Our Process
Using Human-Centered Design
PSI Niger and YLabs joined forces to apply a human-centered design (HCD) approach to develop a tailored intervention which embodied comprehensive community insights into how religious beliefs and health needs can be leveraged to improve support for birth spacing and contraceptive use in Niger.
HCD is is a creative approach to problem solving. It’s about understanding people’s needs, preferences and behaviors to build and prototype solutions that are creative, robust, and informed by the needs of the end user and the implementers. Designers start by understanding the end users’ needs using a variety of ethnographic and observational techniques. Through cultivating curiosity, creativity, systems thinking and exploring lessons from analogous sectors, designers can develop and refine products and services that better engage the target population. By understanding demand drivers for the product or services, insights from the end user are used to iterate and improve the prototypes in order to refine them for implementation and scale.
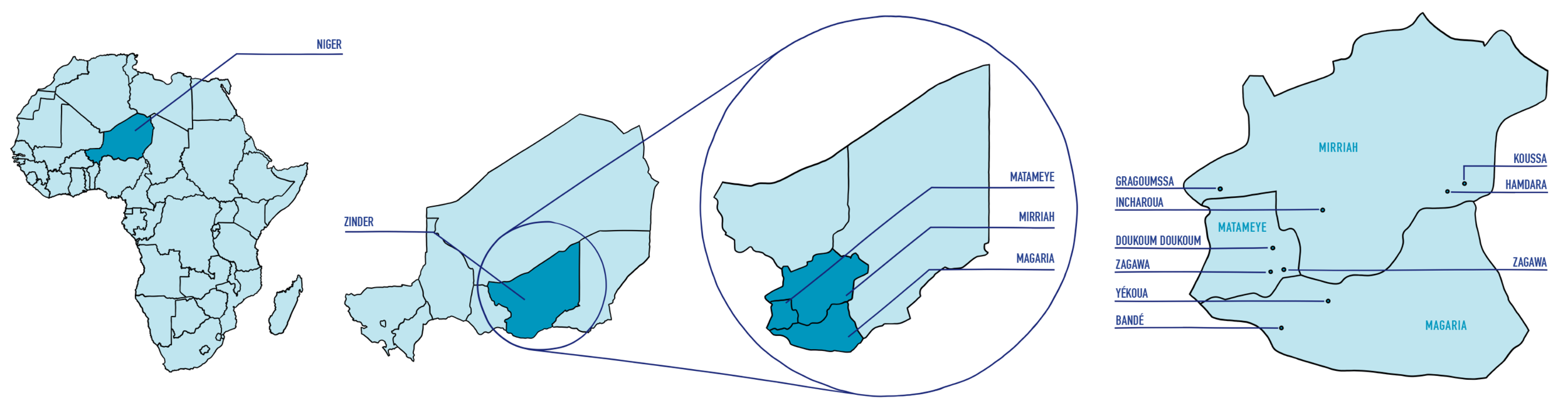
In this HCD process, the team learned a tremendous amount along the way — how to navigate discussions on taboo subjects with sensitivity and care; how to take an intangible idea and turn it into a rough prototype to test; how to use Hausa proverbial expressions to better convey our questions and ideas to our participants in Zinder; and, importantly, how to pivot in our approach when design research revealed surprising and unprecedented findings.
“All our programs are informed by consumer insights. What is different are some of the creative ways that the HCD process gathers these insights. And perhaps even more importantly, how the HCD process quickly designs, tests and iterates the resulting strategies.”
— PSI Representative.